
What Is PTSD? Understanding Trauma, Recovery, and Healing
- Bobby Jakucs, Psy.D.

- 2 days ago
- 13 min read
Updated: 1 day ago
"An abnormal reaction to an abnormal situation is normal behavior.” - Viktor Frankl

This post contains Amazon affiliate links. If you click and make a purchase, I may earn a small commission at no cost to you. These small earnings help fund the mission of the Take Courage Resilience Center and keep the lights on. Thank you for your support.
If you'd like future reflections delivered straight to your inbox—grounded in faith, inspired by classical wisdom, and informed by evidence-based psychology—subscribe here
Viktor Frankl, after surviving the hell of a Nazi concentration camp, once said, “an abnormal reaction to an abnormal situation is normal behavior.” Behind rolls of barbed wire, he, and so many others, witnessed the apotheosis of man’s cruelty. Firing squads, gas chambers, experimental surgeries. Things that exist only in nightmares. Things that defy our ability to grasp.
Trauma has a way of revealing the limits of human reason. It is a shock to our orderly perception of the way the world “should” be. It often leads to profound consequences - psychologically, physiologically and spiritually.
What we now call post-traumatic stress disorder (PTSD) has moved from a diagnostic category to a part of the vernacular. In this series we are going to explore PTSD’s impact on the human person. We are also going to look at what healing looks like.
Editor's Note: This is Part 1 of a three-part series on PTSD. In this article, we'll explore what PTSD is and why it develops. In Part 2 we'll examine what the research says about healing, and in Part 3 we'll explore the existential, spiritual and post-traumatic growth dimensions of recovery.
What is PTSD?
PTSD is defined in the Diagnostic and Statistical Manual of Mental Health Disorders (DSM-5) as, “the development of characteristic symptoms following exposure to one or more traumatic events.” These traumatic events include directly experiencing or witnessing events that include threatened with death, serious injury or sexual violence.
It also includes learning about the details of such instances of a close family member or friend, like a soldier hearing the gruesome details of how his best friend was shot by a sniper. Lastly, it includes repeated or extreme exposure to details of a trauma – such as law enforcement officers having to review the details of child abuse for a case.
PTSD at its core, is as Frankl described, a normal reaction to an abnormal situation. Normal, not in the sense that it is a good thing – far from it - but normal in that it is how our bodies and brains respond when faced threat.
It’s a survival mechanism. It’s the nervous system’s way of ensuring that we are safe from harm. Problems occur when that survival system stays turned on after the initial threat has passed.
The History of PTSD

While we have only recently begun to formally study the effects of trauma, as a species we have experienced those effects since leaving the Garden. Roman philosopher Lucretius detailed legionnaires experiencing nightmares long after leaving the battlefield. He hypothesized it was a result of stress and anxiety. In the Bible, the Book of Job recounts the intense struggles of a man trying to make sense of the loss of his entire family.
Perhaps the oldest recorded trauma reaction occurs in the Epic of Gilgamesh dating back to the third millennium BC. On witnessing the death of his friend Enkidu in battle Gilgamesh says:
“I wept for him seven days and nights, till the worm fastened on him. Because of my brother I am afraid of death, because of my brother I stray through the wilderness. His fate lies heavy upon me. How can I be silent, how can I rest?”
These words could have been spoken by a soldier or Marine returning home today. Often, warriors carry things in their ruck long after the guns fall silent.
With industrialized war in the 19th and 20th century became more significant efforts to understand the phenomena we now call PTSD. In the Civil War, it was called “railway spine” or “soldier’s heart” as soldiers leaving the battlefield were often evacuated by train.
It was believed that this caused an activation of the nervous system leading to cardiovascular issues – heart palpations, sweating, and tremors being the chief symptoms. We’ve since learned that trains were not the cause, but physicians at the times were observing symptoms and doing their best to ascertain the origins.
Alcohol often served as a means to numb the pain. So too opium. Journals and diaries of soldiers and medical professional recount how opium was often prescribed to treat “nervous” symptoms resulting from combat. So much so, it led to an opium epidemic in the 1860s-1870s.
Similarly, in WWI and WWII PTSD was conceptualized as “war neurosis” and “shell-shock” and was believed to be caused by prolonged and intense bombardments so common to those wars. The poet Wilfred Owen, served on the Western Front in WWI and captured the soldier’s experience. In Anthem for Doomed Youth he writes:
What passing-bells for these who die as cattle?
— Only the monstrous anger of the guns.
Only the stuttering rifles' rapid rattle
Can patter out their hasty orisons
Our understanding of PTSD has evolved significantly overtime. But it’s impact on those who experience it has not.
How Common is PTSD?

According to the National Center for PTSD roughly six out of 100 people (6% of the population) will have PTSD at some point in their lives. We say at some point because, yes, PTSD is recoverable.
That statistic is important for two reasons.
First, if you think about how many people are exposed to a traumatic event each year – combat, sexual assault, car accidents, traumatic loss, medical trauma, etc. – only a subset of people each year go on to develop PTSD. That is because we human beings are incredibly resilient.
Every trauma is impactful, but that impact is not always PTSD. Humans have an innate recovery process. If we didn’t, we as a species would have died out long ago.
The second point, trauma hits each person differently. Out of 10 people who experience the same trauma, most will have an acute stress response – the brains way of protecting us from further immediate threat. Most of those individuals will have the innate recovery process kick in and return to baseline. A few will go on to develop more chronic responses to threats that are no longer present – PTSD.
However, line those same 10 people up in a different scenario and those who developed PTSD may be just fine while others who had no issues will go on to struggle.
We all have sensitivities to certain events. Researchers don’t know exactly what causes PTSD in certain individuals. Currently, it is believed to a range of complex and interrelated factors. Further study is underway.
What we do know is that susceptibility does not imply inevitability. Nor does PTSD mean someone is “weak” or “broken.” What it does mean is that they are remarkably human.
Common Symptoms of PTSD
After a traumatic event our nervous system and internal alarm system are heightened. If the system has not returned to baseline naturally (in other words recovered), it remains in fight, flight or freeze mode. This system does not take into account context. Meaning, a soldier returning home from the battlefield, or a child who has been abused and is removed from a dangerous environment, may rationally know they are out of danger. But the body, mind and spirit often don’t.

Intrusive Symptoms
When this occurs the brain has a way of reminding us of what happened so that we can properly orient to threats. We call these intrusive symptoms – where the past breaks into the present. These include recurrent memories, emotional reactions and physical reactions (like sweating, trembling and a racing heart) in the presence of reminders, nightmares and flashbacks.
Avoidance
Avoidance is often called the “hallmark” of PTSD. It is both a symptom, and all too often a way of living. When we are wounded we try to cover ourselves up. We try to avoid anything that will cause pain. So too with wounds that can’t be seen. Unfortunately, we can’t avoid a memory. In fact, when we try to not think about something we invariably have to think about it to make sure we are not thinking about the thing we don’t want to think about. And try as we might we can’t always avoid reminders. So the world starts getting smaller – we’ll explore that more fully soon.
Changes in Mood and Cognitions
We all have a story in our lives, trauma often rewrites that story. I’ve heard many patients say after a trauma that their beliefs about themselves, other people and the world were fundamentally changed. What they thought was true no longer seems to hold weight after the weight of reality comes crashing in. Often, we become fused to our narratives. Description and identity become one and the same.
Hyperarousal
Imagine trying to sleep knowing that a rabid wolf was in your room. Imagine trying to concentrate on a task at work if there was a fire starting in your office. When the internal alarm system remains on, it acts as if danger is still present – even when it has long since passed. It becomes incredibly difficult to sleep even when we are exhausted.
Concentration is impacted. Like a computer with too many programs running – things get slow. All our mental energy is focused on either assessing threats or trying to push back memories. The threshold between frustration and anger is blurred or non-existent. Mind you, anger is an appropriate reaction in context. When faced with a threat it mobilizes us to act. The problem with PTSD is that that anger is often directed at the wrong target.
All of these symptoms are intrinsically linked. They create a self-perpetuating cycle. This cycle can go on for years unchecked. To understand why we’ll need to look at what keeps us stuck in the loop – and how to break it.
PTSD Is Often a Disorder of Non-recovery
Modern PTSD research increasingly points toward a helpful way of understanding the disorder. PTSD is not simply a disorder of fear. It is often best understood as a disorder of non-recovery.
Fear Conditioning
Pain is an incredible teacher. If you have ever touched a hot stove you know. You likely still regularly check the knobs, or gently tap a pot, just to make sure. What has occurred is fear-conditioning. It’s critical for survival. Without this it we would burn our hands all the time – and worse.
The neurobiology underlying fear-conditioning is, as a 2022 meta-analysis states, “among the most well-understood in behavioral neuroscience” with a nearly 30-year research base, including neuroimaging and behavioral studies.
While there are several areas of the brain involved, three predominate. These include:
the amygdala - the nervous system’s alarm and emotion center
the hippocampus - our memory consolidation system
the prefrontal cortex (PFC) - the “executive” center of the brain
The Brain in PTSD
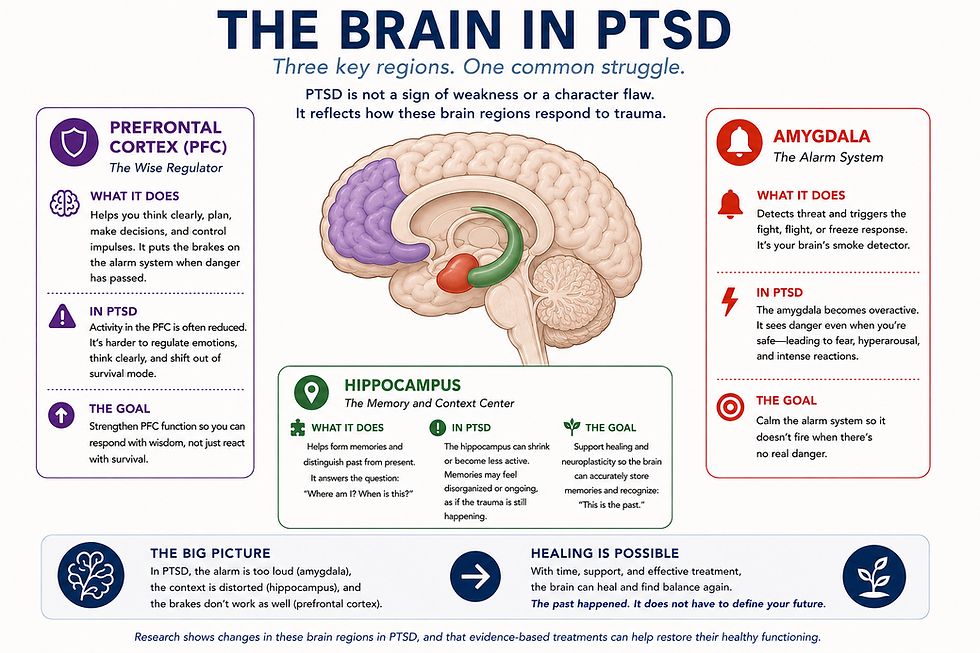
The amygdala’s job is to cue in to threats and trigger the fight, flight or freeze response. The hippocampus helps to place memories in context, such as where and when they occurred. When functioning normally, this allows us to distinguish past danger from present safety. Structurally these two areas are adjacent to each other which is why we learn very quickly not to touch stoves without checking.
In PTSD these two areas fundamentally change. The amygdala becomes over-activated and more sensitive to potential threats. The hippocampus often shows reduced volume on neuroimaging studies or altered functioning, meaning its harder to distinguish past from present.
In the the third area, the PFC neural activity reduced. The PFC takes contextual information from the hippocampus regarding past and present into account to mediate responses. Which is why individuals experiencing PTSD react to triggers even when removed from the environment we first encountered them.
The prefrontal cortex is also like our emotional brakes. It can mediate emotional reactions including fear and anger. From a survival aspect this is all incredibly efficient – our alarm system goes off from a threat (stove) and we immediately remember (pain, check and see if its hot) .
Survival tends to favor speed over accuracy. We don’t want to deliberate whether or not to pull our hand off the hot stove - we just need to pull it off!
Trauma Changes How We Learn

While helpful for preventing kitchen mishaps this becomes problematic when the system is kept on indefinitely. The brain continues to operate under threat conditions. And insidiously it often starts to determine more and more things as threats.
Take a soldier returning home from Iraq or Afghanistan. IEDs were a common. Often, insurgents would hide IEDs in piles of garbage.
Much like the stove, that soldier’s brain quickly learned:
Garbage pile = danger
You might check whether a pan is regardless of whose stove you happen to be using. And that is just from normative learning without the added impact of PTSD. A returning warrior might have that same learned reaction to seeing garbage on the street back home. Because, with the threat system on high alert context is not taken into account.
And it’s not just garbage. Fear conditioning can occur to any sort of stimuli – sights, sounds, smells, people, or even situations.
Take a survivor of sexual assault: suddenly things like a bed or a parking complex are a place of fear and pain. Even when they may be places where the trauma never occurred.
I’ve heard many patients say, regarding their triggers, “I know it’s sounds crazy, Doc, but I just can’t help it. My body responds.” I typically hear those same patients say, “and so I just don’t go near my triggers anymore.”
In other words, “if I avoid things that trigger distress I won’t be distress.” Avoidance sounds great in theory.
But avoidance comes at a profound cost.
How Avoidance Maintains PTSD

Avoidance actually charges you twice. In the first place, when you remove yourself from a situation that causes anxiety your anxiety goes away. That sounds good, right? The problem is the nervous system remembers this. Like ruts forming in a heavily traveled road, it easily becomes the most accessible strategy to cope. Eventually avoidance begins spreading into other areas of life.
Take the Veteran who survived and IED or the woman who survived an assault. The “cant’s” start to add up.
“I can’t be around other people.”
“I can’t be on the road.”
“I can’t sit in a crowded store.”
“I can’t be around another man.”
These “can’t” invariably come up when we try to do what matters: go to work, attend social events, engage in relationships. This then often leads to guilt and thoughts like:
“I’m broken.”
“I’m not the man I used to be.”
“I’ll never be able to trust someone again.”
Also avoidance has a long term cost. Because the brain remembers when we leave a situation, the next time we are faced with a trigger it starts sounding the alarm bells sooner:
“You couldn’t face this then, what makes you think you can face this now?”
Anxiety occurs earlier and more often. So does the urge to avoid that anxiety. It creates a cycle where-in we are more alert to triggers in order to avoid those triggers. And when we avoid those triggers we become even more alert to triggers. Even just the thought of triggers can become triggers themselves.
So far we’ve been taking about external cues in the environment. But there’s another piece. There is a reason we often say people are haunted by their past. Like a specter, memories and thoughts have a way of moving through whatever defenses a person erects.
No matter how hard a person tries, it is impossible to avoid the memories of an unprocessed trauma. It’s like trying to hold a beachball under water. You can only hold it down for so long. Eventually it is going to surface. Often, life becomes about holding back trauma rather than reaching toward what matters.
Anything can serve as an avoidance strategy. In an effort to push out the memories, trauma survivors may drink alcohol or use substances . But those aren’t the only ways. I’ve worked with survivors who overwork, overexercise, overextend, and over-busy themselves in thousands of ways, just to not think about a memory.
And because survivors spend so much time trying to keep the memory buttoned down, those memories become locked into our neural network. They remain wounds that are frozen in time. Wounds that are awakened in the presence of reminders. Or in the silence of night where, like sand castle walls crumbling before the ocean's tide, the mind can no longer distract itself from the flood of memory.
Can PTSD Be Treated? Can People Recover?

The short answer is unequivocally, “yes.” If you read nothing else, please read that sentence again.
The longer answer is, that depends on what you mean by cured. Ultimately, there is no way to erase a memory. But we can recover from them.
Just as the brain learns that something is dangerous, we can relearn that a trigger is in fact safe. We can also learn to not let memories dictate our behaviors. To break the “can’t” cycle and lean into doing what matters.
Trauma makes us learn to be afraid. But changes in neural networks are not etched in stone. We can learn to live again. A 2016 study used neuroimaging to capture this effect. Following PTSD treatment those same areas of the brain (the amygdala, hippocampus and prefrontal cortex) that were altered from fear-based conditioning fundamentally changed. The alarm system down shifted. The PFC started mediating reactions. The brain began the recognize what the person knew intellectually: the danger was over.
Viktor Frankl wrote that, the last of the human freedoms is man’s ability to, “choose his attitude in any given set of circumstances, to choose his own way.” Even when those circumstances include trauma, we can learn to recognize where we have choice. And can find the courage to live again.
Recovery is not simply about reducing symptoms. It is about recovering the freedom to live according to what matters most.
PTSD is very much like an open wound. Avoidance efforts are like bandages someone puts on to try and cover it as best they can. But underneath it remains infected. Wounds can heal if we treat them appropriately. They may leave a scar, but nobody is free from scars.
We need look no further than Christ. After the Resurrection He still bore the wounds of his Crucifixion and death. These were the wounds Thomas demanded to see in order to believe. Christ still bears His wounds. Ultimately, it is in His wounds where ours too can be healed. The soldier-saints like Francis and Ignatius in their own ways demonstrated that not only can wounds heal they can become witness to something more:
Grace. Forgiveness. Love. Mercy. Peace.
Next in the series, we’ll explore what the research shows about how wounds heal.
Additional Resources:
If you'd like to explore these ideas further, here are a few books, organizations and articles I frequently recommend.
Books:
Organizations:
Articles:


